Differences in Users Perception of the Physical Facilities in the First Generation University Teaching Hospitals Southwest, Nigeria
Akinluyi Muyiwa Lawrence1 * , Fadamiro Joseph Akinlabi1 , Falilat Yetunde Olowu 2 and Adeniyi Damilare Akinluyi 3
, Fadamiro Joseph Akinlabi1 , Falilat Yetunde Olowu 2 and Adeniyi Damilare Akinluyi 3
1Department of Architecture, Afe Babalola University, Ado-Ekiti (ABUAD), Nigeria .
2Maintenance Service Department, OAUTHC, Ile-Ife, Osun-State, Nigeria .
3Department of Geography, University of Ibadan (UI), Ibadan, Nigeria .
http://dx.doi.org/10.12944/CRJSSH.8.2.04
This research investigated the variations in how users perceive the physical infrastructure of First Generation University Teaching Hospitals in Southwest Nigeria. As hospitals move beyond their traditional focus on individual care, they are collaborating more with other health sector entities and local communities to make better use of resources and enhance both individual and public health. Since university teaching hospitals are central to healthcare service delivery, gaining insight into how users view their physical environments is essential for service improvement. The research employs a mixed-methods approach, combining quantitative surveys with qualitative interviews to capture a broad range of experiences from patients, healthcare professionals, and administrative staff. At the multivariate analysis stage, a Kruskal-Wallis Post hoc test was applied to the Null Hypothesis H03b to assess whether users’ evaluations of physical facilities including layout, organization, form, circulation, accessibility, visibility, and the number of windows and doors differ across Federal Teaching Hospitals in the region. Findings showed that OAUTHC received higher ratings for physical facilities compared to LUTH and UCH. The paper addresses the practical implications for hospital management and policy, highlighting the importance of focused facility upgrades to improve patient satisfaction, staff efficiency, and overall health outcomes. The study also offers recommendations for both immediate and long-term improvements based on identified challenges.
Copy the following to cite this article:
Lawrence A. M, Akinlabi F. J, Olowu F. Y, Akinluyi A. D. Differences in Users Perception of the Physical Facilities in the First Generation University Teaching Hospitals Southwest, Nigeria. Current Research Journal of Social Sciences and Humanities. 2025 8(2).
DOI:http://dx.doi.org/10.12944/CRJSSH.8.2.04Copy the following to cite this URL:
Lawrence A. M, Akinlabi F. J, Olowu F. Y, Akinluyi A. D. Differences in Users Perception of the Physical Facilities in the First Generation University Teaching Hospitals Southwest, Nigeria. Current Research Journal of Social Sciences and Humanities. 2025 8(2). Available here:https://bit.ly/3LlSX5c
Download article (pdf) Citation Manager Review / Publish History

Introduction
The aim of this study is to assess the physical facilities in Federal University Teaching Hospitals in Southwest Nigeria. Several factors have prompted a renewed examination of hospital design: many facilities built in the mid-20th century are now insufficient for today’s standards of safety and efficiency. Additionally, rapid medical advancements, more complex healthcare needs, and a heightened emphasis on patient- and family-centered care have underscored the urgency of redesigning hospital spaces (Levin & Joseph, 2009; Akinluyi et al., 2021). Well-conceived hospital environments can decrease mistakes, reduce infection rates, prevent injuries, and ease staff workloads. Consequently, there is an increasing call for continual improvements in hospital architecture and interior design. Researchers and designers are striving to create better experiences for all hospital users. Given their key role in the health system, hospitals must be studied through the perspectives of their users, using both qualitative and quantitative approaches (Cifter & Cifter, 2017; Setola et al., 2009; Akinluyi, 2024).
Studies such as Levin and Joseph (2009) demonstrate that thoughtfully designed healthcare spaces can minimize harm, support well-being, and encourage healing. Likewise, Schweitzer et al. (2004) found that the physical environment directly influences patient stress and recovery. As healthcare delivery evolves, facility design is increasingly recognized as a key factor in shaping user experiences. Scholars call for more research into how physical spaces impact user behavior and perception. This study uses an evidence-based approach, drawing on reliable research to inform decisions about hospital environments (Levin & Joseph, 2009; Akinluyi, 2024).
This study seeks to assess the physical design of Federal University Teaching Hospitals in Southwest Nigeria and propose a practical framework for future improvements. Earlier research has prompted a shift among architects, planners, and managers toward connecting building strategies with user satisfaction. While many prior studies (Price & Lu, 2013; Davidson et al., 2007; Verschoren et al., 2015; Nimlyat et al., 2018; Ulrich, 1991; Akinluyi et al., 2019) concentrated on specific design features, this investigation considers both physical and psychological aspects. The objective is to recommend strategies that foster compassionate patient care and a supportive workplace for staff, thereby enhancing hospital performance and patient outcomes.
Specifically, the study tests Hypothesis (H03b), which posits no significant difference in users’ assessments of the physical facilities among Federal University Teaching Hospitals in Southwest Nigeria. The research targeted selected departments of three first-generation Federal University Teaching Hospitals constructed between the 1950s and 1970s: University College Hospital (UCH) Ibadan, Lagos University Teaching Hospital (LUTH), and Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC) Ile-Ife. Departments such as Paediatrics, Internal and Family Medicine, Ophthalmology, Dentistry, and Obstetrics and Gynaecology were included for a comparative analysis of user perceptions.
Literature Review
Studies on Hospital Physical Facilities Design
Srivastava (2017) examined how medical personnel and patients view the architectural design of outpatient clinics and hospitals. Through surveys and interviews, the study assessed aspects like layout, lighting, décor, and their effects on workflow and emotions. The findings revealed that design features impeding movement led to decreased satisfaction, underscoring the importance of thoughtful facility planning. Fawole, Okunlola, and Adekunle (2008) investigated client views on antenatal care quality in both private and public health facilities in Ibadan, looking at elements such as amenities, spacing, cleanliness, ventilation, and utility access. Their results indicated that the quality of physical infrastructure had a significant impact on antenatal care standards. Similarly, Erim, Kolapo, and Resch (2012) evaluated the adequacy of Obstetrics and Gynecology department facilities—including wards, operating rooms, and power supply—and found substantial improvements were needed to reduce maternal mortality in Nigeria.
Steinke (2015) focused on Canadian emergency departments to identify environmental features influencing service experiences. Aspects such as ambiance, user-friendliness, layout, and adaptability were evaluated, with notable dissatisfaction around adaptability and comfort. Amenities were rated average, suggesting emergency department design often fails to meet expectations. Samah, Ibrahim, and Wahab (2013) reviewed the interiors of outpatient facilities, specifically drop-off zones, waiting areas, and consultation rooms, concluding that substantial upgrades were necessary. Lambert et al. (2013) collected feedback from children in Irish hospitals, finding that young patients preferred bright, colorful, comfortable, and imaginative environments, highlighting the importance of child-friendly design. Prahlad et al. (2010) studied patient satisfaction in outpatient departments in Madhya Pradesh, India, considering amenities, staff attitudes, and registration processes, and generally reported positive responses. Andrade et al. (2014) also examined outpatient areas, concluding that thoughtfully designed waiting rooms and entrances improved perceptions of care quality. In a similar study, Tsai et al. (2007) assessed outpatient waiting areas for lighting, seating, cleanliness, and amenities, finding that improvements in these features led to greater comfort. Cho et al. (2004) analyzed the connection between service quality and patient satisfaction in a Korean hospital, focusing on tangible aspects such as waiting areas, equipment, and navigation, and confirmed that these features were closely linked to satisfaction, recommending high standards and dedicated spaces for children.
The Literature Review
Studies on Assessment of the Hospital Physical Facilities Design
Srivastava (2017) explored how both medical staff and patients perceive the architectural design of outpatient clinics and hospitals. Using surveys and interviews, the study gathered insights on aspects such as layout, lighting, décor, and the impact of these elements on workflow and emotional response. It was found that when design features hindered movement, satisfaction decreased, highlighting the importance of thoughtful design in facilitating efficient care and improving patient and staff experiences. Fawole , Okunlola , and Adekunle (2008) focused on how clients viewed the quality of antenatal care in both private and public health facilities in Ibadan. The study considered factors like amenities, spacing, cleanliness, ventilation, and access to basic utilities. Results indicated that the quality of physical facilities strongly influenced the standard of antenatal care provided. Similarly, Erim , Kolapo , and Resch (2012) assessed the adequacy of facilities in an Obstetrics and Gynecology department, including wards, operating rooms, and electricity supply, finding that significant improvements were needed to reduce maternal mortality rates in Nigeria. Steinke (2015) conducted research in Canadian emergency departments to identify which physical environment features contributed to positive service experiences. Aspects such as ambiance, user-friendliness, layout, and adaptability were assessed, with findings showing dissatisfaction, especially regarding adaptability and user comfort. Amenities received average ratings, suggesting that emergency department design often fails to meet user expectations. Samah, Ibrahim, and Wahab (2013) evaluated the interior design of outpatient facilities, focusing on areas like drop-off zones, waiting rooms, and consultation spaces.
They concluded that the design quality was subpar and called for substantial improvements. Lambert et al. (2013) gathered input from children in Irish hospitals, revealing that young patients preferred environments that felt bright, colorful, comfortable, and imaginative, emphasizing the need for child-friendly design features. Prahlad et al. (2010) assessed patient satisfaction in outpatient departments in Madhya Pradesh, India, considering elements such as amenities, staff attitudes, and the registration process. Their findings suggested general satisfaction with the facilities provided. Andrade et al. (2014) also examined the physical environment of hospital outpatient areas and found that well-designed waiting rooms and entrances significantly improved patients’ perceptions of service quality. In a similar vein, Tsai et al. (2007) looked at outpatient waiting areas in a medical center, evaluating aspects like lighting, seating, cleanliness, and access to amenities. They found that enhancements in these areas positively affected the overall environment and patient comfort. Cho et al. (2004) investigated the link between service quality and patient satisfaction in a Korean hospital, focusing on tangible elements such as the waiting area, equipment quality, and ease of navigation. The study confirmed that patients’ perceptions of these physical features were closely tied to their overall satisfaction, recommending that clinics maintain high standards and consider dedicated spaces for children.
The Study Area
Nigeria is organized into six geo-political zones: South-South, South-East, South-West, North-Central, North-West, and North-East. This research focused on the South-West zone, recognized as a leader in healthcare advancement within the country. The region is home to the nation’s first-generation Federal University Teaching Hospitals (FUTH), which were established between the 1950s and 1970s. The South-West comprises six states Oyo, Osun, Ekiti, Ogun, Ondo, and Lagos. However, this study specifically centers on Oyo, Osun, and Lagos States, where these pioneering hospitals are situated: University College Hospital (UCH) in Ibadan, Lagos University Teaching Hospital (LUTH) in Lagos, and Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC) in Ile-Ife.
University College Hospital (UCH) in Ibadan, Oyo State, was founded in 1952 under an Act of Parliament to address the need for training healthcare professionals in Nigeria and the wider West African region. Officially opened on November 20, 1957, and designed by Mr. Alexander Gray (F.R.I.B.), the original facility featured six main blocks and 493 beds. Initially launched with 500 beds, UCH has since expanded to a capacity of 850 beds, accommodating over 6,000 outpatient visits annually. The hospital hosts multiple departments and specialties, such as Ophthalmology, Paediatrics, Family Medicine, Internal Medicine, Obstetrics and Gynaecology, and Surgery.
Lagos University Teaching Hospital (LUTH), located in the Idi-Araba area of Surulere in Lagos State, was established in July 1962. The hospital started with 330 beds and has grown to a capacity of 761 beds, serving more than 9,000 outpatients each year. LUTH, like UCH, provides a broad spectrum of specialized services, including Ophthalmology, Paediatrics, Family Medicine, Internal Medicine, Obstetrics and Gynaecology, and Surgery.
Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC) in Ile-Ife, Osun State, was conceived as the clinical arm of the Obafemi Awolowo University medical school, inaugurated in July 1975. Spanning latitudes 7°30’0.0’’ to 7°31’6.71’’N and longitudes 4°33’0.0’’ to 3°34’30.64’’E, OAUTHC is grounded in a philosophy of integrated healthcare. It offers primary, secondary, and tertiary care, aiming to enhance the physical, mental, and socio-economic wellbeing of Nigerians. The complex boasts 547 beds distributed across 25 departments, providing an array of services in Paediatrics, Family Medicine, Internal Medicine, Ophthalmology, Obstetrics and Gynaecology, and Surgery.
Table 1: Federal University Teaching Hospitals in Southwest Nigeria
S/N | Hospital Name | Year of | State Located | Town | Manager |
1 | University College Hospital (UCH), Ibadan, Oyo-state | 1952 | Oyo | Ibadan | Federal Government |
2 | Lagos University Teaching Hospital (LUTH), Idi-Araba, Lagos-State | 1962 | Lagos | Lagos | Federal Government |
3 | Obafemi Awolowo University Teaching Hospital (OAUTHC), Ile-Ife, Osun-State | 1975 | Osun | Ile-Ife | Federal Government |
Sources: Author Field Survey, 2019
Materials and Methods
This research adopted a mixed-methods approach for data collection, as detailed below:
Quantitative Survey
The study targeted two main groups: (1) users of hospital physical facilities including staff members, inpatients, and outpatients and (2) the physical buildings within the three Federal University Teaching Hospitals in Southwest Nigeria (UCH in Ibadan, LUTH in Lagos, and OAUTHC in Ile-Ife). Data regarding staff and hospital structures were sourced from the administrative records of each hospital, while patient numbers were determined based on bed counts and outpatient records from December 2019 to December 2020. Altogether, the study considered 39,787 users and 198 buildings.
The sampling frame consisted of both users and buildings from four core departments such as Medicine, Paediatrics, Surgery, and Obstetrics & Gynaecology in each hospital. This resulted in user counts of 468 at UCH, 538 at LUTH, and 241 at OAUTHC (a combined total of 1,247). For buildings, 45 departmental structures were included: 18 at UCH, 11 at LUTH, and 16 at OAUTHC.
Sample sizes were determined using the Krejcie and Morgan (1970) formula, resulting in 210, 217, and 148 user samples for UCH, LUTH, and OAUTHC, respectively, for a total of 575 questionnaires. Staff and patient samples at each hospital were allocated proportionally. For buildings, sampling was restricted to four core departmental buildings in each hospital that accommodate 4 main departments which gave birth to other departments and also carried out pure clinical activities for medical treatment. These departments are Paediatrics, Surgery, Medicine, Obstetrics and Gynaecology (See table 2.0). A stratified sampling technique was used for users, first categorizing respondents as either staff (clinical and non-clinical) or patients (inpatient and outpatient), followed by random selection within these groups.
The structured questionnaire consisted of sections designed to address the study’s research questions, objectives, and hypotheses. Three versions were developed: Type A for staff, Type B for inpatients, and Type C for outpatients. In total, 575 questionnaires were distributed 204 to staff and 371 to patients. The questionnaire items were based on operational definitions of variables (see Table 3.0), including codes, categories, Likert scale ranges, measurement scales, and analysis tools. Variables were selected from existing literature and previous studies, with Type A including most items from Types B and C.
Responses from the structured questionnaires were analyzed using descriptive statistics, such as frequency distributions, weighted means, and standard deviations. At the bivariate level, Kendall’s tau-b correlation was used to explore relationships between design features of physical facilities. For multivariate analysis, the Kruskal-Wallis Post hoc test was employed to test the Null Hypothesis H03b, which states that there are no significant differences in users’ assessments of physical facilities across the three hospitals.
Qualitative Interview
Semi-structured interviews were conducted on days with lighter clinical workloads typically Mondays and Wednesdays with key personnel, including department heads, consultants, matron nurses, and maintenance managers or architects/engineers. Access to conduct these interviews and collect relevant data was granted through formal approval from the management of each selected hospital.
Table 2 : Sampling Frame, Sample Size and Percentages of sample selected
USERS (STAFF & PATIENTS) | |||||||
S/N | Teaching Hospitals | Sampling Frame | Sample Size | No of Staff Selected | % of Staff Selected | No of Patients Selected | % of Patient Selected |
1 | University College Hospital, Ibadan (UCH), Oyo State. | 468 | 210 | 79 | 37.6 | 131 | 62.4 |
2 | Lagos University Teaching Hospital (LUTH), Lagos State | 538 | 217 | 73 | 33.6 | 144 | 66.3 |
3 | Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife (OAUTHC), Osun State. | 241 | 148 | 52 | 35.1 | 96 | 65.0 |
Total Sample Size for Users | 1,247 | 575 | 204 | 106.3 | 371 | 193.7 | |
BUILDING STRUCTURES | |||||||
S/N | Teaching Hospitals | Sampling Frame | Sample Size | ||||
1 | University College Hospital, Ibadan (UCH), Oyo State. | 18 | 4 | ||||
2 | Lagos University Teaching Hospital (LUTH), Lagos State | 11 | 4 | ||||
3 | Obafemi Awolowo University Teaching Hospital Complex, Ile-fe (OAUTHC), Osun State. | 16 | 4 | ||||
Total Sample Size for Building | 45 | 12 | |||||
Source: Study area records office, 2019 (Between the periods of December 2019- December 2020), Krejcie and Morgan (1970)
Table 3: Operationalisation of variables and Measurement scales for the research
S/N | Description of Variables | Variable Codes | Categories of | Measurement Scale | Range of Scale | Analytical Tools |
1 | Layout of the Buildings and Spaces | LAYBS | 1. Strongly dissatisfied; 2. Dissatisfied 3. Fair 4. Satisfied 5.Strongly satisfied | Ordinal | 1-5 | Frequency and Percentage, weighted mean and standard deviation, Kendal tau-b, Kruskal Wallis (H)test |
2 | Organization of Interior Spaces & Furniture | ORGISF | 1. Strongly dissatisfied; 2. Dissatisfied 3. Fair; 4. Satisfied 5.Strongly satisfied | Ordinal | 1-5 | Frequency and Percentage, weighted mean and standard deviation, Kendal tau-b, Kruskal Wallis (H)test |
3 | Form/Shape of Building & Spaces | FOSH-BS | 1. Strongly dissatisfied; 2. Dissatisfied 3. Fair 4. Satisfied ; 5.Strongly satisfied | Ordinal | 1-5 | Frequency and Percentage weighted mean and standard deviation, Kendal tau-b, Kruskal Wallis (H)test |
3 | Movement Pattern/Flow within the Interior Spaces | M-FLOW | 1. Strongly dissatisfied; 2. Dissatisfied 3. Fair 4. Satisfied ; 5.Strongly satisfied | Ordinal | 1-5 | Frequency and Percentage, weighted mean and standard deviation, Kendal tau-b; Kruskal Wallis (H)test |
4 | Accessibility to Building and Interior Spaces | AC-BIS | 1. Strongly dissatisfied; 2. Dissatisfied 3. Fair 4. Satisfied ; 5.Strongly satisfied | Ordinal | 1-5 | Frequency and Percentage; weighted mean and standard deviation; Kendal tau-b, Kruskal Wallis (H)test |
5 | Visibility within the interior spaces | VIS-INT | 1. Strongly dissatisfied; 2. Dissatisfied 3. Fair 4. Satisfied 5.Strongly satisfied | Ordinal | 1-5 | Frequency and Percentage, weighted mean and standard deviation, Kendal tau-b and Kruskal Wallis (H)test |
6 | Number of Windows & Doors | SIZE-NW | 1. Strongly dissatisfied; 2. Dissatisfied 3. Fair 4. Satisfied ; 5.Strongly satisfied | Ordinal | 1-5 | Frequency and Percentage; weighted mean and standard deviation and Kendal tau-b and Kruskal Wallis (H)tes |
Results
Quantitative Survey
A Kruskal-Wallis Post hoc test was conducted to investigate the significant difference in the users' assessment of physical facilities among the Federal Teaching Hospital in Southwest, Nigeria. The results of the differences in the physical facilities are discussed in the section below from the Null Hypothesis H03b.
Difference in Layout of the Building and Space at the FUTH
A significant difference was observed in users’ assessments of the layout of the building and space among the Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria. This analysis was conducted to determine whether users’ evaluations of physical facilities varied across the three study areas. The results, presented in Table 4.0 and Figure 1.0, indicate that the null hypothesis is rejected at a P-value of 0.000, which is less than the 0.05 significance level. The mean rank assessments of the physical facilities are as follows: Obafemi Awolowo University Teaching Hospital Complex (OAUTHC): 344.62, University College Hospital (UCH): 287.10 and Lagos State University Teaching Hospital (LUTH): 224.69. These rankings are presented in descending order of user satisfaction. To further identify the level of statistical significance in the differences, a Kruskal-Wallis post hoc test was performed. The test revealed statistically significant pairwise differences between all three hospitals:
LUTH vs. UCH
LUTH vs. OAUTHC
UCH vs. OAUTHC
All comparisons showed P-values < 0.05, confirming significant variations in the assessment of building layouts and spaces.
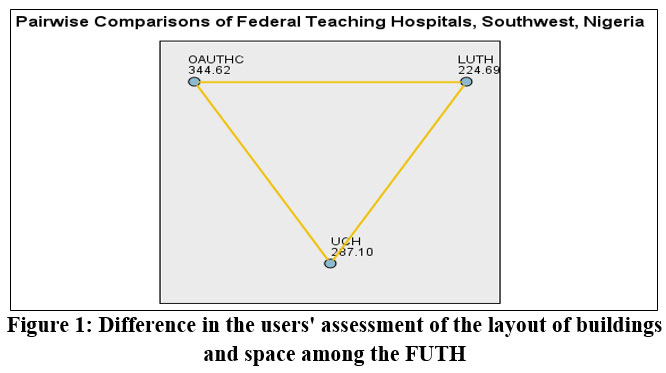 | Figure 1: Difference in the users' assessment of the layout of buildings and space among the FUTH |
Table 4: Difference in the users' assessment of the layout of buildings and space among the FUTH
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -62.411 | 15.554 | -3.984 | .000 | .000 |
LUTH-OAUTHC | -119.934 | 17.305 | -6.930 | .000 | .000 |
UCH-OAUTHC | 57.523 | 17.25 | 3.334 | .000 | .003 |
source: Researcher’s Field Survey, 2021.
Difference in Organisation of the interior spaces and furniture at the FUTH
This analysis examined differences in the organisation of interior spaces and furniture across the three Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria. The null hypothesis stated that there is no significant difference in users’ assessments of the interior space and furniture organisation among the three hospitals. However, the results revealed that the null hypothesis is rejected at a P-value of 0.000, which is less than the 0.05 (5%) significance level. The mean rank assessments are as follows: Obafemi Awolowo University Teaching Hospital Complex (OAUTHC): 342.07, University College Hospital (UCH): 289.52 and Lagos State University Teaching Hospital (LUTH): 224.02. These values, as shown in Figure 2.0, indicate significant differences in user satisfaction levels regarding the interior space and furniture across the hospitals.
Furthermore, Table 5.0 presents the results of post hoc pairwise comparisons, which confirm statistically significant differences in user assessments between all pairs:
LUTH vs. OAUTHC
LUTH vs. UCH
UCH vs. OAUTHC
Each comparison yielded a P-value of 0.000, indicating strong statistical significance.
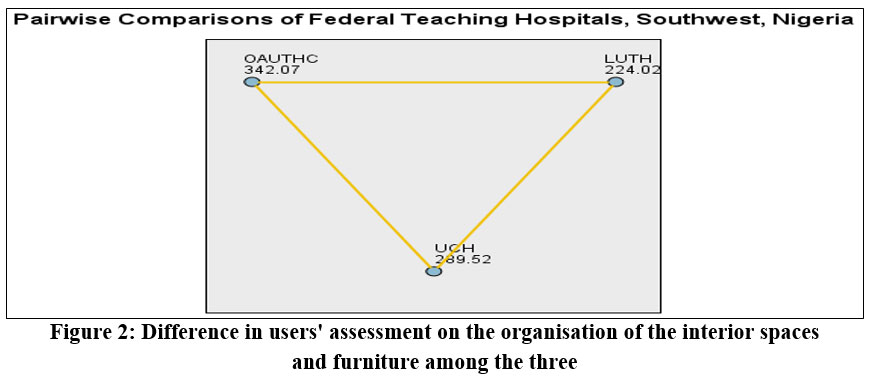 | Figure 2: Difference in users' assessment on the organisation of the interior spaces and furniture among the three. |
Table 5: Difference in users' assessment on the organisation of the interior spaces and furniture
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -65.497 | 15.701 | -4.172 | .000 | .000 |
LUTH-OAUTHC | -118.042 | 17.345 | -6.805 | .000 | .000 |
UCH-OAUTHC | 52.544 | 17.295 | 3.038 | .002 | .007 |
Each row tests the null hypothesis that the Samples 1 and 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is .05. | |||||
Source: Researcher’s Field Survey, 2021
Difference in the Form/shape of building and spaces at the FUTH
The difference in the form and shape of the buildings and spaces across the three Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria was analysed using the Kruskal-Wallis post hoc test. The results revealed a statistically significant difference in users’ assessments of the form and shape of the buildings and spaces among the three hospitals. This indicates that the form/shape of the buildings and spaces is not uniform across the study areas. As presented in Table 6.0 and Figure 3.0, the mean rank scores were: Obafemi Awolowo University Teaching Hospital Complex (OAUTHC): 347.12, University College Hospital (UCH): 280.07, and Lagos State University Teaching Hospital (LUTH): 230.06
The pairwise comparison results showed statistically significant differences as follows:
LUTH vs. UCH: P = 0.04
LUTH vs. OAUTHC: P = 0.000
UCH vs. OAUTHC: P = 0.000
Since all p-values are less than 0.05, the null hypothesis is rejected, confirming that significant differences exist in the form and shape of buildings and spaces across the three FUTHs.
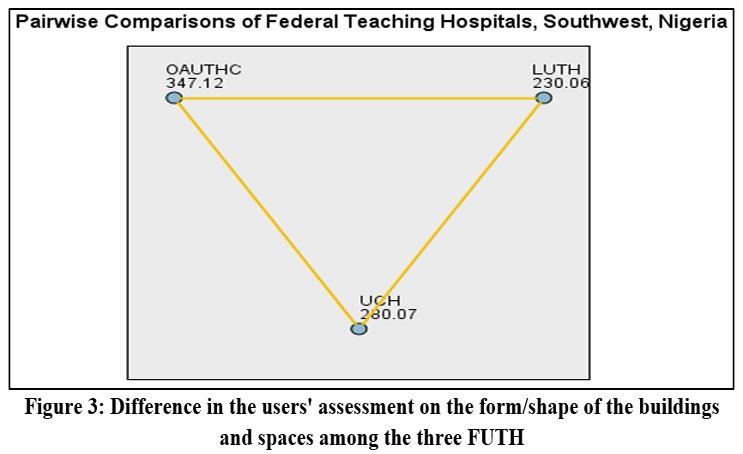 | Figure 3: Difference in the users' assessment on the form/shape of the buildings and spaces among the three FUTH |
Table 6: Difference in the users' assessment of the form/shape of the buildings and spaces
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -50.004 | 15.635 | -3.198 | .001 | .004 |
LUTH-OAUTHC | -117.062 | 17.274 | -6.777 | .000 | .000 |
UCH-OAUTHC | 57.048 | 17.223 | 3.894 | .000 | .000 |
Each row tests the null hypothesis that the Samples 1 and 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is .05. | |||||
Source: Researcher’s Field Survey, 2021
Difference in Movement Pattern/flow within the Interior Spaces at the FUTH
This analysis examined the pattern of movement within the interior spaces of the three Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria: LUTH, OAUTHC, and UCH. The objective was to determine whether there is a statistically significant difference in the interior movement flow across the three hospitals.
The null hypothesis which states that there is no significant difference in the movement patterns was rejected, as the analysis yielded a P-value of 0.000, which is less than the 0.05 significance level. The mean rank scores for user assessments of movement patterns within the hospitals were as follows: Obafemi Awolowo University Teaching Hospital Complex (OAUTHC): 357.6, University College Hospital (UCH): 271.43, and Lagos State University Teaching Hospital (LUTH): 231.46.
These values, illustrated in Figure 4.0, indicate that movement within the interior spaces varies significantly among the hospitals. A pairwise comparison (as shown in Table 7.0) further confirmed significant differences:
LUTH vs. UCH: P = 0.030
LUTH vs. OAUTHC: P = 0.000
UCH vs. OAUTHC: P = 0.000
These results confirm the presence of statistically significant differences in the flow of movement within the interior spaces of the three FUTHs.
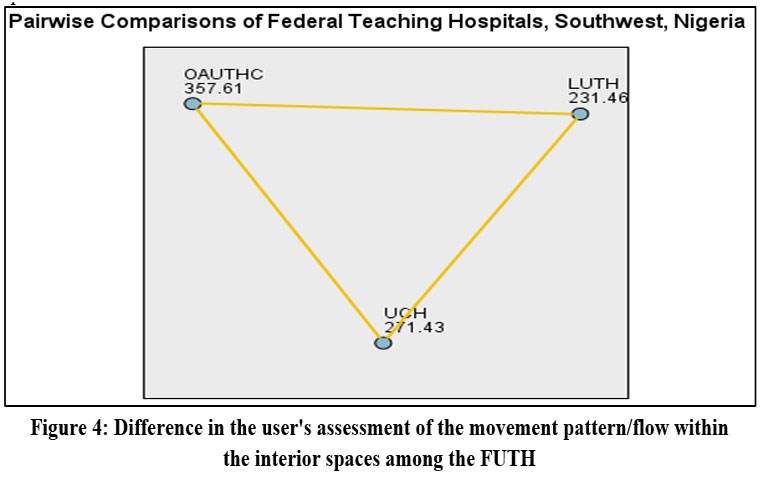 | Figure 4: Difference in the user's assessment of the movement pattern/flow within the interior spaces among the FUTH. |
Table 7: Difference in the user's assessment of the movement pattern/flow within the interior spaces
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -39.967 | 15.549 | -2.570 | .010 | .030 |
LUTH-OAUTHC | -126.154 | 17.179 | -7.343 | .000 | .000 |
UCH-OAUTHC | 86.187 | 17.128 | 5.032 | .000 | .000 |
Each row tests the null hypothesis that the Samples 1 and 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is .05. | |||||
Source: Researcher’s Field Survey, 2021.
Difference in Accessibility to Building and Interior Spaces at the FUTH
To examine the differences in accessibility to buildings and interior spaces across the Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria, a Kruskal-Wallis H test was conducted. This test assessed whether there were statistically significant differences in users' assessments of physical facility accessibility among the three hospitals. As shown in Table 8.0, the result indicates that the null hypothesis is rejected, with a P-value of 0.000, which is less than the 0.05 significance level. This confirms a statistically significant difference in accessibility to buildings and interior spaces among the hospitals. The mean rank scores, as illustrated in Figure 5.0, are: Obafemi Awolowo University Teaching Hospital Complex (OAUTHC): 360.19, University College Hospital (UCH): 278.40, and Lagos State University Teaching Hospital (LUTH): 222.58
Further pairwise comparisons revealed significant differences between the following pairs:
LUTH vs. UCH: P = 0.01
LUTH vs. OAUTHC: P = 0.000
UCH vs. OAUTHC: P = 0.000
These values confirm that the accessibility conditions vary significantly across the three FUTHs in Southwest Nigeria.
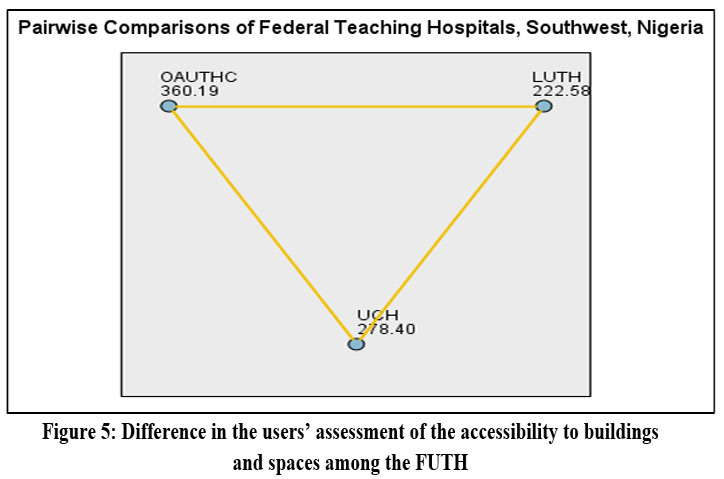 | Figure 5: Difference in the users’ assessment of the accessibility to buildings and spaces among the FUTH |
Table 8: Difference in the users’ assessment of the accessibility to buildings and spaces
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -55.826 | 15.698 | -3.556 | .000 | .001 |
LUTH-OAUTHC | -137.615 | 17.343 | -7.935 | .000 | .000 |
UCH-OAUTHC | 81.790 | 17.292 | 4.730 | .000 | .000 |
Each row tests the null hypothesis that the Samples 1 and 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is .05. | |||||
Source: Researcher’s Field Survey, 2021.
Difference in Visibility within the Interior Space at the FUTH
Visibility within the interior space was examined as a critical factor in users’ assessment of physical facilities across the three Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria. The aim was to determine whether a statistically significant difference exists in visibility assessments among the hospitals. As presented in Table 9.0, the null hypothesis which states that there is no significant difference in visibility was rejected, with a P-value of 0.000, which is less than the 0.05 (5%) significance level. This confirms that there is a statistically significant difference in users' assessment of interior space visibility across the study areas. The mean rank scores for visibility are as follows (as shown in Figure 6.0): Obafemi Awolowo University Teaching Hospital Complex (OAUTHC): 357.09, University College Hospital (UCH): 266.54 and Lagos State University Teaching Hospital (LUTH): 236.80.
These rankings suggest varying levels of visibility satisfaction among users.
A pairwise comparison using the Kruskal-Wallis post hoc test yielded the following results:
LUTH vs. UCH: P = 0.161 (not significant)
LUTH vs. OAUTHC: P = 0.000 (significant)
UCH vs. OAUTHC: P = 0.000 (significant)
These findings indicate that while LUTH and UCH are not statistically different in terms of visibility, both differ significantly from OAUTHC.
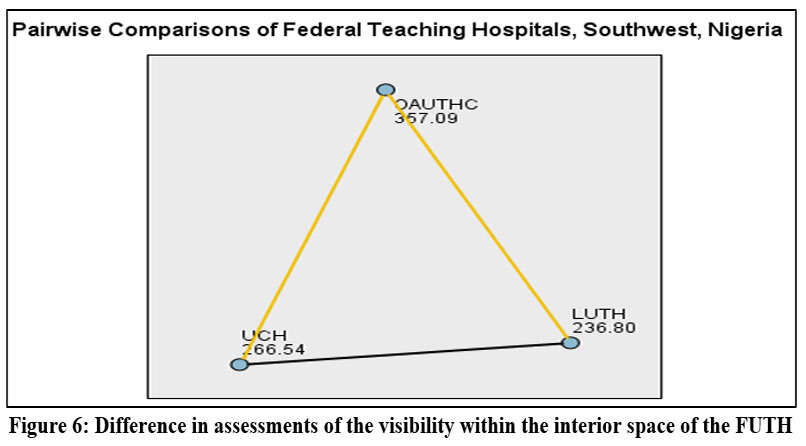 | Figure 6: Difference in assessments of the visibility within the interior space of the FUTH |
Table 9: Difference in assessments of the visibility within the interior space
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -29.741 | 15.411 | -1.930 | .054 | .161 |
LUTH-OAUTHC | -120.292 | 17.027 | -7.065 | .000 | .000 |
UCH-OAUTHC | 90.551 | 16.976 | 5.334 | .000 | .000 |
Each row tests the null hypothesis that the Samples 1 and 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is .05. | |||||
Source: Researcher’s Field Survey, 2021.
Difference in Numbers of Windows and Doors within the interior space at the FUTH
The number of windows and doors within interior spaces was examined as a key design measure in the assessment of physical facilities across the Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria. The objective was to determine whether a statistically significant difference exists in the provision of these elements among LUTH, UCH, and OAUTHC.
Using the Kruskal-Wallis post hoc test, the analysis revealed that the null hypothesis is rejected at a P-value < 0.05, indicating a statistically significant difference in the number of windows and doors among the three hospitals. To further identify specific group differences, pairwise comparisons were conducted, as shown in Table 10.0:
LUTH vs. UCH: P = 0.359 ? Not statistically significant
LUTH vs. OAUTHC: P = 0.000 ? Statistically significant
UCH vs. OAUTHC: P = 0.000 ? Statistically significant
The mean rank scores, presented in Figure 7.0, indicate the following:
OAUTHC: 344.31
UCH: 268.25
LUTH: 244.04
These mean ranks highlight varying levels of user satisfaction regarding the quantity and distribution of windows and doors in the hospitals.
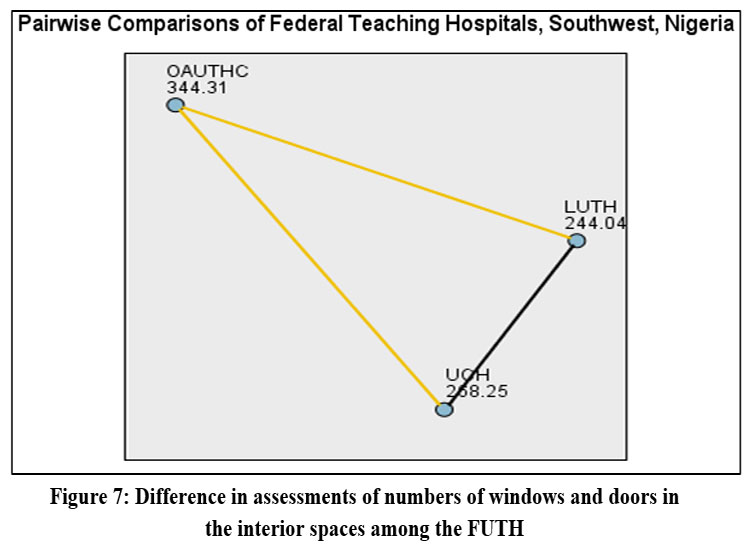 | Figure 7: Difference in assessments of numbers of windows and doors in the interior spaces among the FUTH. |
Table 10: Difference in assessments of numbers of windows and doors in the interior spaces
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -24.206 | 15.551 | -1.930 | .120 | .359 |
LUTH-OAUTHC | -100.267 | 17.181 | -5.836 | .000 | .000 |
UCH-OAUTHC | 76.060 | 17.129 | 4.440 | .000 | .000 |
Each row tests the null hypothesis that the Samples 1 and 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is .05. | |||||
Source: Researcher’s Field Survey, 2021.
Difference in Users' Assessment of the Physical Facilities at the FUTH
The physical facilities of the Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria were assessed using seven design-related variables:
Layout of buildings and spaces
Organisation of interior spaces and furniture
Form/shape of buildings and spaces
Movement pattern/flow within interior spaces
Accessibility to buildings and interior spaces
Visibility within interior spaces
Number of windows and doors within interior spaces
These variables served as the design criteria for evaluating the performance of physical facilities across the three hospitals: LUTH, UCH, and OAUTHC.
The primary objective of the analysis was to test the null hypothesis that there is no significant difference in users' assessments of physical facilities across the hospitals. According to the decision rule, if P-value < 0.05, the null hypothesis is rejected.
As shown in the hypothesis testing results, the null hypothesis was rejected at P-value < 0.05, indicating that there is a statistically significant difference in the users’ assessment of physical facilities among the three hospitals.
The mean rank scores (illustrated in Figure 8.0) were:
OAUTHC: 364.80
UCH: 287.10
LUTH: 224.69
These results confirm that OAUTHC received the highest overall assessment, followed by UCH, and then LUTH. Additionally, a Kruskal-Wallis post hoc test was conducted to examine pairwise differences among the hospitals. The results, as presented in Table 11.0, show that all three pairings LUTH vs. UCH, LUTH vs. OAUTHC, and UCH vs. OAUTHC produced P-values < 0.05, confirming statistically significant differences in all comparisons.
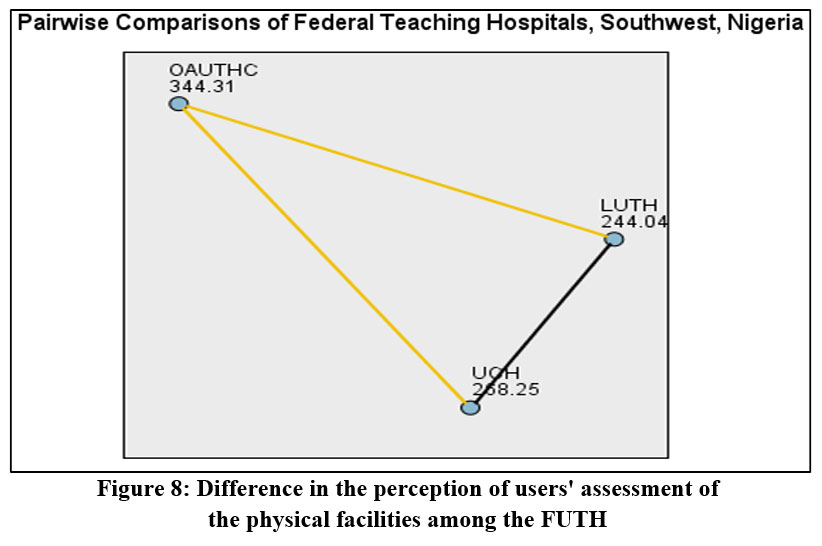 | Figure 8: Difference in the perception of users' assessment of the physical facilities among the FUTH |
Table 11: Difference in the users' assessment of the physical facilities
Each node shows the sample average rank of the FUTH, Southwest, Nigeria | |||||
Sample 1-Sample 2 | Test Statistics | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. |
LUTH-UCH | -61.741 | 15.831 | -3.869 | .000 | .000 |
LUTH-OAUTHC | -146.292 | 17.491 | -8.380 | .000 | .000 |
UCH-OAUTHC | 85.551 | 17.439 | 4.892 | .000 | .000 |
Each row tests the null hypothesis that the Samples 1 and 2 distributions are the same. Asymptotic significances (2-sided tests) are displayed. The significance level is .05. | |||||
Source: Researcher’s Field Survey, 2021.
The Difference in the users’ assessment of the Physical Facilities at the FUTH
The users’ assessments of physical facilities at the Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria were analyzed based on seven key variables such Layout of buildings and spaces, Organisation of interior spaces and furniture, Form/shape of buildings and spaces, Movement pattern/flow within interior spaces, Accessibility to buildings and interior spaces, Visibility within interior spaces and Number of windows and doors. The results for each variable are summarized below and presented in Table 12.0. The result for layout of the buildings and spaces show that UCH shows the chi-square X2(cal) = 257.98; Mean rank = 356.82, and p-value = 0.002; LUTH (chi-square X2(cal) = 262.48; Mean rank = 342.67, and p-value = 0.012), and OAUTHC (chi-square X2(cal) = 203.882; Mean rank = 396.45, and p-value = 0.000). For organisation of interior spaces and furniture in UCH (chi-square X2(cal) = 121.65; Mean rank = 311.75, and p-value = 0.000); LUTH (chi-square X2(cal) = 147.220; Mean rank = 299.79, and p-value = 0.003), and OAUTHC (chi-square X2(cal) = 117.05; Mean rank = 331.89.10, and p-value = 0.000).
Forms/Shape of building and spaces for UCH shows the value of chi-square X2(cal) = 129.146; Mean rank = 299.99 and p-value = 0.005; LUTH (chi-square X2(cal) = 121.061; Mean rank = 289.11, and p-value = 0.000) and OAUTHC (chi-square X2(cal) = 154.880; Mean rank = 305.18, and p-value = 0.000). The fourth variable which is the movement pattern/flow within the interior spaces shows the result of the UCH (chi-square X2(cal) = 217.910; Mean rank = 378.56, and p-value = 0.004; LUTH (chi-square X2(cal) = 218.593; Mean rank = 386.19, and p-value = 0.000), and OAUTHC (chi-square X2(cal) = 247.272; Mean rank = 396.05, and p-value = 0.000).
Accessibility to building and interior space for UCH (chi-square X2(cal) = 135.130; Mean rank = 344.13, and p-value = 0.002 ); LUTH (chi-square X2(cal) = 140.225; Mean rank = 312.32, and p-value = 0.000), and OAUTHC (chi-square X2(cal) = 152.259; Mean rank = 365.17, and p-value = 0.001); visibility within the interior spaces for OAUTHC (chi-square X2(cal) = 217.275; Mean rank = 277.13, and p-value = 0.000); LUTH (chi-square X2(cal) = 215.829; Mean rank = 298.902, and p-value = 0.000), and UCH (chi-square X2(cal) = 259.902.061; Mean rank = 281.30, and p-value = 0.001). The last variable considered is the number of windows and doors in the three FUTH. For number of windows and doors in OAUTHC, the result of the analysis shows the value of chi-square X2(cal) = 117.242; Mean rank = 259.10, and p-value = 0.003; LUTH (chi-square X2(cal) = 152.858.061; Mean rank = 276.54, and p-value = 0.000) and UCH (chi-square X2(cal) = 117.231; Mean rank = 244.13, and p-value = 0.001).
The findings however indicate that OAUTHC performs better than LUTH and UCH in the aspect of the layout of buildings and spaces; organisation of interior spaces and furniture; form/shape of building and spaces; movement pattern/flow within the interior spaces and accessibility to building and interior spaces while LUTH performs better than OAUTHC and UCH when considering the visibility within the interior spaces and the number of windows and doors within the interior space.
Table 12: Difference in the users’ assessment of the Physical Facilities in the FUTH
Variables | Differences in the Physical Facilities at the FUTH, Southwest, Nigeria | |||||||||||
UCH | LUTH | OAUTHC | ||||||||||
Chi-square | DF | Mean rank | P-value | Chi-square | DF | Mean rank | P-value | Chi-square | DF | Mean rank | P-value | |
LAYBS | 257.98 | 2 | 356.82 | 0.002 | 262.48 | 2 | 342.67 | 0.012 | 203.882 | 2 | 396.45 | 0.000 |
ORGISF | 121.65 | 2 | 311.75 | 0.000 | 147.220 | 2 | 299.79 | 0.003 | 117.05 | 2 | 331.89 | 0.000 |
FOSH-BS | 129.146 | 2 | 299.99 | 0.005 | 121.061 | 2 | 289.11 | 0.000 | 154.880 | 2 | 305.18 | 0.000 |
M-FLOW | 217.910 | 2 | 378.56 | 0.004 | 218.593 | 2 | 386.19 | 0.000 | 247.272 | 2 | 396.05 | 0.000 |
AC-BIS | 135.130 | 2 | 344.13 | 0.002 | 140.225 | 2 | 312.32 | 0.000 | 152.259 | 2 | 365.17 | 0.001 |
VIS-INT | 217.275 | 2 | 277.13 | 0.000 | 215.829 | 2 | 298.44 | 0.000 | 259.902 | 2 | 281.30 | 0.001 |
SIZE-NEW | 117.242 | 2. | 259.10 | 0.003 | 152.858 | 2 | 276.54 | 0.000 | 117.231 | 2 | 244.13 | 0.001 |
LAYBS=Layout of the buildings and spaces, ORGISF=Organization of interior spaces and furniture, FOSH-BS= Form/shape of building and spaces, M-FLOW= Movement pattern/flow within the interior spaces, AC-BIS = Accessibility to building and interior spaces, VIS-INT =Visibility within the interior spaces and SIZE-NEW =Number of windows and doors
Source: Researcher’s Field Survey, 2021.
Testing of Hypothesis 3 (H03b)
Hypothesis 3 (H03b) was tested using the Kruskal-Wallis test to evaluate whether there is a statistically significant difference in users' assessments of physical facilities among the three Federal University Teaching Hospitals (FUTHs) in Southwest Nigeria: OAUTHC, UCH, and LUTH.
The null hypothesis (H?) states
There is no significant difference in the users’ assessment of the physical facilities among the three FUTHs in Southwest Nigeria.
The decision rule is as follows:
If the p-value is less than 0.05 (5% significance level), reject the null hypothesis; otherwise, do not reject it.
As presented in Table 13.0, the analysis yielded a p-value = 0.000, which is less than 0.05, and therefore, the null hypothesis is rejected. This result implies that there is a statistically significant difference in users’ assessments of physical facilities among OAUTHC, UCH, and LUTH, with a confidence level of approximately 95%.
Table 13: Kruskal-Wallis Test: Users’ assessment of the Physical Facilities among the FUTH
Chi-square | df | F (2,554) | P-value | |
Users’ assessment of the physical facilities | 70.220 | 2 | 0.000 |
Where *** indicates P-value < 0.01, ** indicates P-value < 0.05, and ** indicates P-value < 0.1. Grouping variable: Federal University Teaching Hospitals in the southwest (OAU, UCH, and LUTH).
Source: Researcher’s Field Survey, 2021.
Discussion of the Study
The findings of this study reveal that both staff and patients perceive notable differences in the layout and spatial organization of the three hospitals examined. The null hypothesis was rejected at the 5% significance level, indicating that these variations are statistically significant rather than random. Of the three hospitals, OAUTHC achieved the highest mean rank, reflecting more positive evaluations of its spatial layout and arrangements. UCH ranked second, while LUTH received the lowest scores, suggesting greater dissatisfaction with its spatial design. These outcomes suggest that the architectural planning at OAUTHC is more attuned to user needs, potentially due to better navigation, zoning, or circulation pathways. This aligns with Joseph (2006), who highlighted the impact of well-structured layouts on reducing stress and enhancing efficiency in healthcare settings. The results point to a need for redesigning the layouts at UCH and, in particular, LUTH to foster better user experience and satisfaction. This is further supported by Reiling (2008), who noted that effective spatial planning can decrease adverse incidents and improve safety.
Significant differences were also reported regarding the organization of interior spaces and furniture. Again, OAUTHC led in user satisfaction, suggesting superior interior layout and ergonomics, while UCH followed, and LUTH lagged behind. These results reinforce the argument by Schweitzer, Gilpin, and Frampton (2004) that interior design including ergonomic furniture and spatial arrangement plays a direct role in patient recovery, staff performance, and overall wellness. The findings underscore the need for interior design upgrades at LUTH and UCH to provide more functional and healing-oriented environments.
Analysis of the form and shape of the hospital buildings revealed similar trends. OAUTHC was rated most favorably for its architectural form, with UCH receiving moderate scores and LUTH the lowest. This suggests that OAUTHC’s design offers a more effective combination of aesthetics and functionality. Levin (2007) also observed that the physical form of healthcare buildings influences user satisfaction, safety, and institutional image. Future improvements at UCH and LUTH should therefore consider architectural enhancements that blend visual appeal with practical utility, echoing Joseph & Rashid (2007), who emphasized that well-defined spatial layouts can serve as barriers to accidents and bolster safety.
When it comes to movement and traffic flow within the hospitals, OAUTHC again outperformed the others, suggesting more efficient circulation and easier navigation. Lower scores at LUTH indicate challenges with internal movement, which corresponds with Ulrich et al. (2008), who emphasized the value of intuitive circulation patterns in reducing patient stress and improving staff workflow. Enhancing wayfinding and movement in UCH and LUTH could yield improvements in both satisfaction and operational effectiveness.
Accessibility was another area where OAUTHC excelled, followed by UCH, with LUTH again trailing. Features like ramps, lifts, wide corridors, and clear signage were reportedly better at OAUTHC. These findings are consistent with universal design concepts (Mace, 1998), which advocate for accessible environments to increase inclusivity and functional outcomes in healthcare. The results highlight the urgent need for accessibility improvements at LUTH and UCH.
OAUTHC also received higher ratings for visibility within its spaces, likely due to better lighting, openness, and visual pathways. UCH and LUTH performed similarly but less favorably. This supports Verderber and Fine (2000), who noted the importance of visibility and natural lighting for comfort, safety, and wayfinding in hospitals.
With respect to windows and doors, OAUTHC was again rated best, attributed to better natural light, ventilation, and accessibility. While LUTH performed comparably to UCH in this area, both were rated below OAUTHC. Ulrich (1991) highlighted the significant role of access to daylight and fresh air in patient recovery and satisfaction, indicating that UCH and LUTH should focus on improving these features.
Overall, the study demonstrates statistically significant differences in users’ assessments of physical facilities among the three hospitals. OAUTHC’s higher performance is likely influenced by its more recent construction (1975) compared to UCH (1957) and LUTH (1962), and possibly by ongoing renovations and upgrades, as suggested by Ulrich et al. (2008), which are vital for keeping pace with modern healthcare demands.
While OAUTHC generally outperformed the other hospitals, LUTH showed relative strengths in visibility and environmental comfort, possibly due to its emphasis on windows and doors, reflecting the importance of natural light and ventilation (Ulrich, 1991). UCH ranked in between, with moderate performance across most variables.
In summary, the results confirm substantial differences in user perceptions of physical facilities across the three teaching hospitals. The findings highlight the need for targeted infrastructural improvements—especially at LUTH and UCH in areas such as spatial layout, accessibility, and circulation, while preserving advantages in natural lighting and ventilation. Ongoing evaluation and modernization are crucial to keep hospital environments aligned with best practices (Levin, 2007; Joseph, 2006), thereby enhancing user satisfaction and healthcare outcomes.
Results from the Qualitative Interview
Structured questionnaires were distributed to patients with the assistance of clinical staff directly involved in their care, as well as to other staff groups, with the support of a trained team of field assistants. These assistants received comprehensive training on the correct procedures for administering questionnaires, including appropriate locations, timing, and methods, and worked under the researcher’s direct supervision.
The research team consisted of twenty field assistants, comprising assistant lecturers, ten senior instructors, and 400-level Architecture students from Joseph Ayo Babalola University, Ikeji-Arakeji, Osun State. They were deployed to the study sites for three weeks.
Questionnaires were administered on designated clinical days such as Tuesdays, Thursdays, and Fridays between 8:00 a.m. and 4:00 p.m., ensuring the participation of all respondent groups across the selected departments.
In addition to the surveys, semi-structured interviews were conducted to further evaluate the physical facilities in Federal University Teaching Hospitals in Southwest Nigeria. The following outline was used as a guide for these interviews:
Interview Guide
Name of the University Teaching Hospital: …………………………………………
Status of the Respondent: …………………………………………
(e.g., Doctor – Consultant, Resident, House Officer; Nurse – Matron, Nursing Officer, Student Nurse)
What are your views about the physical facilities in your hospital generally?
How do you perceive your wards/clinical spaces, considering the following features?
Layout and organization of the buildings and interior spaces
Form/shape of the building and interior spaces
Movement and visibility within the interior spaces
Accessibility to buildings and interior spaces
Number and size of components within the interior spaces, such as windows and doors (height and width).
The result from the qualitative content analysis were displaced below in the table 14.0;
Table 14: Typical Transcripts (Contents Analysis) For Semi-Structured Interview (SSI) Discussion for the FUTH, South-West, Nigeria
S/N | Question | Answer Given (LUTH) | Answer Given (UCH) | Answer Given (OAUTHC) |
1 | What are your views about the Physical Facilities in your hospital generally? | The hospital buildings are generally good as the management carries out periodic renovations. However, they are only moderately okay, requiring further redesign and upgrading. Overall, the facilities can be described as fair, with moderate stability and purpose-driven within available resources. | The structures are old, with some already dilapidated and long overdue for upgrades. While facilities are satisfactory, maintenance is inadequate. | Physical facilities are old and many are non-functional. They are not strategically located for easy accessibility and are generally below standard. |
2a | Perception of wards/clinical spaces: Layout & Organization of the Buildings and Interior Spaces | The hospital layout is fairly good but interior spaces require better organization for improved functionality and productivity. Some wards and clinical spaces are poorly organized, though the theatres were purpose-built and conducive. | The layout of the wards and clinical spaces is good but could be further improved for better use. Overall, interior organization is adequate and satisfactory. | Layout and organization are only average and not in the best state. Improvements are needed to enhance efficiency. |
2b | Form/Shape of Building & Interior Spaces | The external form and shape of the buildings are good. However, interior arrangements require improvement. While the form is commendable, materials used in interior spaces are substandard. | Building shapes are good, and the interior spaces are moderately okay. Overall, the form and shape of the spaces are adequate and satisfactory. | The form and shape of the buildings and interior spaces are only fair and average. |
2c | Movement & Visibility within the Interior Spaces | Movement within wards and clinical spaces is generally conducive for both patients and staff. Visibility during the day and night is good. However, difficulties are experienced in certain areas such as surgical wards. | Movement and visibility are limited, partly due to adjustments during the COVID-19 pandemic. Nonetheless, spaces are spacious enough to allow free movement with adequate visibility. | Movement flow patterns and visibility within wards and clinical spaces are satisfactory. |
2d | Accessibility to Building and Interior Spaces | Accessibility to both hospital buildings and departments is generally good, with adequate labeling of spaces. However, some areas still require improvement. | Accessibility is satisfactory, with most areas having proper entry points and pathways. | Accessibility to hospital buildings and interior spaces is satisfactory and considered very good. |
2e | Number & Size of Windows and Doors (height & width) in wards, clinical spaces, waiting areas | Window and door sizes are generally adequate in terms of height and width, allowing vision and easy movement of equipment. However, many are stiff, rusted, and difficult to open, requiring frequent maintenance or replacement. | Sizes of windows and doors are generally adequate, though cross ventilation is often poor, leading to stuffy conditions in crowded spaces such as outpatient departments. | Windows and doors in clinical and waiting areas are well-constructed and adequate in size. Ventilation is generally satisfactory. |
Source: Researcher’s Field Survey, 2021.
Conclusion
This research demonstrates that users’ evaluations of physical facilities vary significantly among the three Federal University Teaching Hospitals (FUTH) in Southwest Nigeria, as shown by both bivariate and multivariate analyses. OAUTHC consistently achieved the highest ratings in key design elements, including building layout, spatial organization, architectural form, movement flow, and accessibility. In contrast, LUTH was rated above both OAUTHC and UCH in terms of interior visibility and the number of windows and doors.
Further analysis using post hoc tests affirmed OAUTHC’s leading performance in the overall assessment of physical environments. This advantage is likely linked to the hospital’s more recent establishment in 1975, as opposed to LUTH (1962) and UCH (1957). The older institutions appear to face challenges related to aging infrastructure and may be less equipped to cope with increasing healthcare demands. In comparison, OAUTHC has benefited from regular maintenance, renovations, and new construction, allowing it to better fulfill modern healthcare needs.
The variation in the age, design philosophy, and upkeep of these facilities explains the differences in user satisfaction observed across the hospitals. The findings highlight the vital role of ongoing infrastructure upgrades and adaptive architecture in improving user experience within healthcare settings.
Results from the structured questionnaires revealed that many respondents indicated a willingness to recommend the hospital to friends or other potential users. However, some participants interviewed through the Semi-Structured Interviews (SSI) at FUTH expressed reservations. They reported that they were not fully satisfied with the current state of the hospital and would only recommend its physical facilities if significant improvements were made particularly in staff efficiency, patient health outcomes, and the reduction of disease and germ transmission.
In summary, OAUTHC emerges as the most satisfactory hospital for physical infrastructure, followed by LUTH, with UCH ranking lowest, reflecting both the strengths and the limitations of older hospital designs.
The Study Recommendations
Based on the evaluation of physical facilities at the three FUTH in Southwest Nigeria, and given OAUTHC’s consistent superiority in architectural and spatial aspects, the following steps are recommended:
Upgrade Design Standards
Hospital architects, planners, and facility managers should systematically review and modernize the design standards at LUTH and UCH. Special emphasis should be placed on improving layout, spatial arrangement, accessibility, and internal circulation. Adopting user-focused and evidence-based design principles will enhance both functionality and satisfaction for all users.
Government Support
The Federal Government of Nigeria, through the Ministry of Health and related agencies, should make the revitalization of aging infrastructure at LUTH and UCH a priority. This should involve comprehensive renovation, rehabilitation, and reconstruction programs, as well as the construction of new buildings to expand capacity and improve service quality.
Sustained Maintenance
Establishing a culture of continuous maintenance and periodic modernization is crucial for all FUTH. Instituting a robust maintenance framework will preserve the quality of hospital facilities and support better patient experiences, higher staff productivity, and improved healthcare outcomes.
Ultimately, implementing these recommendations will enable LUTH and UCH to better align with modern healthcare delivery standards and meet the growing demands of Nigeria’s urban populations.
Acknowledgement
The author would like to thank the Federal University of Technology, Akure, Ondo-State for granting the Ph.D. research work. The Department of Architecture, School of Environmental Technology, Maintenance Unit of OAUTCH, My supervisor and The research institute of the of the University for their guidance during the course of study.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
The manuscript incorporates all datasets produced or examined throughout this research study.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Permission to Reproduce Material Permission to Reproduce Material from Other Sources
Not Applicable
Author Contributions
Muyiwa Lawrence Akinluyi: Conceptualization of the research Idea, Methodology, Writing and Original Draft.
Falilat Yetunde Olowu : Questionnaire and interview Administration, Data Collection and Resource
Fadamiro Joseph Akinlabi: Visualization, Supervision, Project Administration, Review & Editing.
Adeniyi Damilare Akinluyi : Data Collection, Analysis, Writing and Resources.
References
- Akinluyi, M. L. (2024). Analysis of the morphological design features of the hospital physical facilities in Southwest, Nigeria. XXVII International Scientific Conference on Advance in Civil Engineering “Construction of the Formation of Living Environment” (FORM-2024), E3S Web of Conferences, 533, 02034, 1–19. https://doi.org/10.1051/e3sconf/202453302034
CrossRef - Akinluyi, M. L., Awe, F. C., Adeleye, O. O., & Ogunruku, M. P. (2019). Paediatric physical facilities design characteristics in Southwestern Nigerian university teaching hospital: Lesson from Netherland children hospital. Universal Journal of Public Health, 7(6), 233–254. https://doi.org/
CrossRef - Akinluyi, M. L., Fadamiro, J. A., Ayoola, H. A., & Alade, M. J. (2021). Design quality and level of compliance for out-patient physical facilities: Lesson for hospital developers in Southwest, Nigeria. International Journal of Research and Innovation in Social Science (IJRISS), 5(2), 554. https://www.rsisinternational.org
- Akinluyi, M. L., Fadamiro, J. A., Ayoola, H. A., & Alade, M. J. (2021). Theoretical issues and conceptual framework for physical facilities design in hospital buildings. Journal of Architectural Environment & Structural Engineering Research, 4(1), 28–35. https://doi.org/10.30564/jaeser.v4i1.2240
CrossRef - Andrade, C. C., Lima, M. L., Devlin, A. S., & Hernández, B. (2014). Is it the place or the people? Disentangling the effects of hospitals’ physical and social environments on well-being. Environment and Behavior, 48(2), 299–323.
CrossRef - Cho, W. H., Lee, H., Kim, C., Lee, S., & Choi, K. S. (2004). The impact of visit frequency on the relationship between service quality and outpatient satisfaction: A South Korean study. Health Services Research, 39, 13–33. https://doi.org/10.1111/j.1475-6773.2004.00213.x
CrossRef - Cifter, A. S., & Cifter, M. (2017). A review on future directions in hospital spatial designs with a focus on patient experience. The Design Journal, 20(sup1), S2999–S3008. https://www.tandfonline.com/loi/rfdj20
CrossRef - Davidson, P., Rhéaume, A., Dykeman, M., Ericson, P., Duffett-Leger, L., & Doucet, J. (2007). Nurses' voice: Influencing the restructuring of the New Brunswick healthcare system. Canadian Journal of Nursing Leadership, 20(3), 100–114. https://doi.org/10.12927/cjnl.2007.19474
CrossRef - Erim, D. O., Kolapo, U. M., & Resch, S. C. (2012). A rapid assessment of the availability and use of obstetric care in Nigerian healthcare facilities, 7, 1–8.
CrossRef - Fawole, A. O., Okunlola, M. A., & Adeyemi, O., Adekunle, A. O. (2008). Clients’ perceptions of the quality of antenatal care. Journal of the National Medical Association, 100(9), 1052–1058.
CrossRef - Joseph, A. (2006). The impact of the environment on infections in healthcare facilities. The Center for Health Design.
- Joseph, A., & Rashid, M. (2007). The architecture of safety: Hospital design. Current Opinion in Critical Care, 13(6), 714–719. https://doi.org/10.1097/MCC.0b013e3282f1be6e
CrossRef - Lambert, V., Coad, J., Hicks, P., & Glacken, M. (2013). Young children’s perspectives of ideal physical design features for hospital-built environments. Journal of Child Health Care, 18(1), 57–71.
CrossRef - Levin, D. J., & Joseph, A. (2009). Planning, design, and construction of health care facilities (2nd ed.). Joint Commission on Accreditation of Healthcare Organizations.
- Levin, S. (2007). Designing for safety: Evidence-based design’s impact on patient safety. The Center for Health Design.
- Mace, R. L. (1998). Universal design in housing. Assistive Technology, 10(1), 21–28. https://doi.org/10.1080/10400435. 1998.10131955
CrossRef - Nimlyat, P. S., Anumah, J. J., Odoala, M. C., & Benjamin, G. K. (2018). Spatial distribution of the nature of indoor environmental quality in hospital ward buildings in Nigeria. In Indoor Environmental Quality (pp. 1–32). IntechOpen.
- Prahlad, R. S., Rajeev, K. K., Jayati, S., & Laxman, S. (2010). Measuring patient satisfaction: A case study to improve quality of care at public health facilities. Indian Journal of Community Medicine, 35(1), 5.
CrossRef - Price, A. D. F., & Lu, J. (2013). Impact of hospital space standardization on patient health and safety. Architectural Engineering and Design Management, 9, 49–61.
CrossRef - Samah, Z. A., Ibrahim, N., & Wahab, M. H. (2013). Users’ assessment on interior environment of a hospital outpatient unit in Malaysia. Asian Journal of Environment-Behaviour Studies, 4(11), 73–83.
- Setola, N. (2009). A new approach to the flows system analysis in the teaching hospitals. In D. Koch, L. Marcus, & J. Steen (Eds.), Proceedings of the 7th International Space Syntax Symposium (pp. 099:1–099:7). Stockholm: KTH.
- Schweitzer, M., Gilpin, L., & Frampton, S. (2004). Healing spaces: Elements of environmental design that make an impact on health. Journal of Alternative & Complementary Medicine, 10(1), S71–S83. https://doi.org/10.1089/1075553042245953
CrossRef - Srivastava, C. (2017). Effect of clinic design on patient care: Perceptions of medical staff and patients. Intersect, 10(2).
- Steinke, C. (2015). Assessing the physical service setting: A look at emergency departments. Health Environments Research & Design Journal, 8, 31–42.
CrossRef - Tsai, C. Y., Wang, M. C., Liao, W. T., Lu, J. H., Sun, P. H., Lin, B. Y., & Breen, G. M. (2007). Hospital outpatient perceptions of the physical environment of waiting areas: The role of patient characteristics on atmospherics in one academic medical center. BMC Health Services Research, 7, 198. https://doi.org/10.1186/1472-6963-7-198
CrossRef - Ulrich, R. (1991). Effects of interior design on wellness: Theory and recent scientific research. Journal of Healthcare Interior Design, 3, 97–109.
- Ulrich, R. S., Quan, X., Zimring, C., Joseph, A., & Choudhary, R. (2008). The role of the physical environment in the hospital of the 21st century: A once-in-a-lifetime opportunity. The Center for Health Design.
- Verschoren, L., Annemans, M., Steenwinkel, I. V., & Heylighen, A. (2015). How to design child-friendly hospital architecture? Young patients speaking. In Proceedings of the 3rd European Conference on Design4Health, 13–16 July, Sheffield-Hallam University, Sheffield.
- Verderber, S., & Fine, D. J. (2000). Healthcare architecture in an era of radical transformation. Yale University Press.

This work is licensed under a Creative Commons Attribution 4.0 International License.




